- “Contact area” is a term used to denote the proximal heights of contour of the mesial and distal surfaces of the tooth.1
- A well-contoured, properly positioned, firm proximal contact is essential to maintain the integrity of the dental arches and the health of the supporting structures.
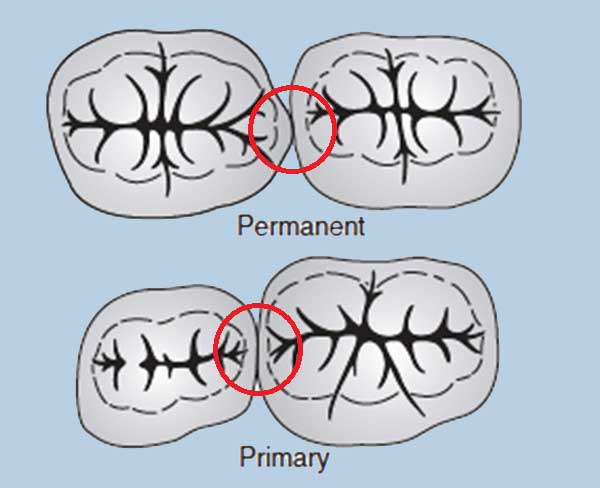
- The existing textbooks in pediatric dentistry suggest contact areas between primary molars are broader, flatter, and situated farther gingivally than the contact points between permanent molars. 1-4
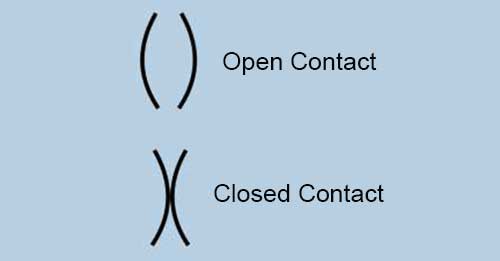
- A review of literature in this area reveals the presence of two types of contacts - open & closed. 6-11
- The authors have suggested that the risk for approximal caries in the posterior primary dentition is increased if contact points are closed rather than open. 6,8
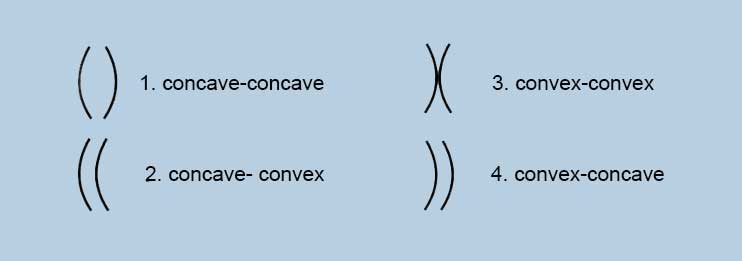
Cortes A et al. described four approximal variants, 12
They concluded that that the morphology of approximal surfaces in primary molar teeth, particularly when both surfaces were concave, significantly influenced the risk of caries development
There is evidence to state that broad proximal contact areas seen in primary teeth are likely to increase caries susceptibility. This could be attributed to the reduction in the mechanical cleansing action, leading to greater plaque accumulation. 4,5
References
- Kennedy DB. Anatomy of primary and permanent teeth. In: Pediatric Operative Dentistry. Kennedy DB, eds. 3rd ed. Bristol, UK:IOP Publishing Limited; 1986:37.
- Mathewson RJ, Primosch RE. Morphology of the primary teeth. In: Fundamentals of Pediatric Dentistry. Mathewson RJ, Primosch RE, eds. 3rd ed. Batavia, Ill., USA: Quintes-sence Publishing Co.; 2014:197.
- Muthu MS, Sivakumar N. Chronology and morphology of primary and permanent teeth. In: Pediatric Dentistry: Principles and Practice. Muthu MS, Sivakumar N, eds. 2nd ed. Batavia, Ill., USA: Elsevier; 2011:33.
- Waggoner WF. Restorative dentistry for the primary dentition. In: Pediatric Dentistry: Infancy Through Adolescence. Casamassimo PS, Fields HW, McTigue DJ, Nowak AJ, eds. 5th ed. Batavia, Ill., USA: Elsevier; 2005:34.
- Gohil KS, Talim ST, Singh I. Proximal contacts in posterior teeth and factors influencing interproximal caries. J Prosthet Dent 1973;30(3):295-302.
- Allison PJ, Schwartz S. Interproximal contact points and proximal caries in posterior primary teeth. Pediatr Dent 2003;25(4):334-40.
- Parfitt GJ. Conditions influencing the incidence of occlusal and interstitial caries in children. J Dent Child 1956;23:31-9.
- Subramaniam P, Babu KG, Nagarathna J. Interdental spacing and dental caries in the primary dentition of 4- to 6-year-old children. J Dent (Tehran) 2012;9(3):207-14.
- Warren JJ, Slayton RL, Yonezu T, Kanellis MJ, Levy SM. Interdental spacing and caries in the primary dentition. Pediatr Dent 2003;25(2):109-13.
- Berman DS, Slack GL. Caries progression and activity in approximal tooth surfaces: A longitudinal study. Br Dent J 1973;134(2):51-7.
- Dean JA, Barton DH, Vahedi I, Hatcher EA. Progression of interproximal caries in the primary dentition. Clin Pediatr Dent 1997;22(1):59-62.
- Cortes A, Martignon S, Qvist V, et al.: Approximal morphology as predictor of approximal caries in primary molar teeth.
Clin Oral Invest. 2018; 22(2): 951–9.